Methodological Note for The Economic Cost of Gun Violence
You can’t put a price on the lives that are altered or cut short each year by gun violence. But gun-related violence in the United States—40,000 deaths and 76,000 more shot and wounded in an average year—has a steep economic cost. This Note is a companion to The Economic Cost of Gun Violence.
As survivors and their loved ones, community members, employers, and taxpayers, we suffer the economic consequences of $557 billion annually for a set of key costs and losses related to the aftermath of gun violence, whether the shooting was unintentional, an assault or homicide, a police-involved shooting, or an act of suicide. These costs, both immediate and long-term, include such items as medical bills, ambulance and patient transport, police response and investigations, criminal justice costs, work loss from forgone earnings, and quality-of-life lost to gun violence each year.
Everytown for Gun Safety Support Fund worked with the leading health economist researching the cost of gun violence, Ted R. Miller, and other researchers at the Pacific Institute for Research and Evaluation (PIRE), notably David I. Swedler and Bruce A. Lawrence, as well as Kathryn Schnippel Bistline and Erica Jade Mullen, to update PIRE’s costing model of the economic cost of gun violence in the United States. PIRE’s well-documented Injury Cost Model1Bruce A. Lawrence et al., “The Consumer Product Safety Commission’s Revised Injury Cost Model,” Pacific Institute for Research and Evaluation, February 2018, https://www.cpsc.gov/s3fs-public/ICM-2018-Documentation.pdf; Bruce A. Lawrence and Ted R. Miller, “Quality of Life Loss Estimation Methods for the WISQARS Cost of Injury Module,” Pacific Institute for Research and Evaluation, January 2020, https://www.cdc.gov/injury/wisqars/pdf/pire_wisqars_cost_injury_quality_life_loss_estimation_methods-508.pdf. has been used to estimate the societal costs of medical treatment, work loss, and quality of life loss resulting from fatal and nonfatal firearm injuries by state. The medical and work-loss components of the Injury Cost Model form the backbone of the CDC’s Web-based Injury Statistics Query and Reporting System (WISQARS) injury costs2The CDC’s online tool—WISQARS Cost of Injury—uses 2020 fatal injuries from the CDC and 2020 nonfatal injuries from the National Electronic Injury Surveillance System–All Injury Program (NEISS-AIP) operated by the US Consumer Product Safety Commission. This tool generates different results from those presented here because it omits some information on nonfatal firearms hospitalizations. In the face of increasing scrutiny of the reliability of this data, the CDC has not published complete information on firearms injuries on its website. Everytown for Gun Safety strongly supports equipping the CDC with the funds necessary to thoroughly measure and examine gun violence. used to calculate the costs of injuries in the United States from a variety of different causes, including, but not limited to, firearms.
PIRE estimates the costs of firearm injury (both fatal and nonfatal) as the product of the cost per injury or death times the number of injured or killed (see Figure 1).
Figure 1. Calculating the cost of gun violence
The cost framework of PIRE’s Injury Cost Model presents costs to the government, paid for by taxpayers, and costs and losses to society. The economic cost to society includes three types of costs: direct expenses, work-loss (indirect) costs, and quality-of-life (intangible) costs. In addition to the costs included in the Injury Cost Model, mental health care, police investigations and response, court costs, incarceration, and perpetrator work-loss costs were also added to the total economic cost calculation presented in this work using the methodology described below. All costs are presented in 2019 dollars using the consumer price and employment cost indices from the US Bureau of Labor Statistics.3US Bureau of Labor Statistics “12-Month Percentage Change, Consumer Price Index, Selected Categories (Past 20 Years),” accessed March 21, 2022, https://bit.ly/3qUBT7r; US Bureau of Labor Statistics, “Employment Cost Index – December 2019,” news release, January 31, 2020, https://www.dol.gov/newsroom/economicdata/eci_01312020.pdf.
For the calculation of costs by state, national average unit costs were used. There is no adjustment for state-by-state cost-of-living differences, differential hospitalization costs by state, or differential rates and lengths of incarceration for assault perpetrators. Per resident state costs were generated by dividing state costs by the total 2019 state population obtained from the US Census Bureau. Likewise, taxpayer costs were generated dividing state costs by 2019 data on all residents 18 and older from the US Census Bureau.
Calculating Firearm Deaths and Injuries
Firearm deaths. PIRE obtained the number of firearm deaths from the CDC’s Multiple Cause of Death data for 2019, the most recent year of data available at the time of analysis. Firearm deaths were identified through the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10). Counts of 10 or fewer are suppressed by the CDC to protect victim and family privacy.4Data from 2019. Centers for Disease Control and Prevention, National Center for Health Statistics, Division of Vital Statistics, Multiple Cause of Death data.
ICD-10 cause codes included are:5World Health Organization, International Statistical Classification of Diseases and Related Health Problems, 10th Revision (Geneva: World Health Organization, 2012), https://icd.who.int/browse10/2016/en.
- W32–W34 (accidental discharge of firearms)
- X72–X74 (suicide by discharge of firearms)
- X93–X95 (homicide by discharge of firearms)
- Y22–Y24 (discharge of firearms, undetermined intent)
- Y35.0 (legal intervention involving firearm discharge)
- U01.4 (terrorism involving firearms)
Nonfatal firearm injuries. PIRE used emergency department and inpatient nationwide sample datasets from the US Department of Health and Human Services’ Healthcare Cost and Utilization Project (HCUP) from 2019, the most recent year of data available at the time of publication.6Nationwide Emergency Department Sample (NEDS) and National Inpatient Sample (NIS), both part of the Healthcare Cost and Utilization Project (HCUP) of the US Department of Health & Human Services’ Agency for Healthcare Research and Quality (AHRQ). Data are from 2019, the most recent year available for this analysis. Since the emergency department HCUP dataset is a sample based on 38 states, PIRE also obtained hospital discharge census data from a subset of state health departments. They then compared the state emergency department census data to the HCUP sample data, and generated modeled estimates using both sources. PIRE’s resultant injury total is slightly higher than the total derived directly from HCUP, but still falls within the 95 percent confidence interval for the HCUP injury total.
Nonfatal injuries include only those that resulted in a hospital visit, whether in the emergency department or an inpatient. They do not include untreated firearm injuries or injuries only treated in a physician’s office or urgent care clinic.
Nonfatal firearm injuries were identified through ICD-10-Clinical Modification (ICD-10-CM) codes for initial visits that paralleled the ICD-10 codes listed above. Counts of 10 or fewer are suppressed. For further details on the methodology of estimating nonfatal injuries by state, see here.
In reporting firearm costs by state, PIRE combined unintentional and undetermined intent into a single category (unintentional/undetermined intent) as per the detailed definitions and coding instructions from the CDC.7Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, “Definitions for Nonfatal Injury Reports,” July 19, 2019, https://www.cdc.gov/injury/wisqars/nonfatal_help/definitions_nonfatal.html. Homicide, legal intervention (i.e., shootings by police), and terrorism were also combined into a single category (homicides/assaults/shootings by police) because many shootings by police are incorrectly coded as assault and homicide.8Andrew Conner et al., “Validating the National Violent Death Reporting System as a Source of Data on Fatal Shootings of Civilians by Law Enforcement Officers,” American Journal of Public Health 109, no. 4 (February 21, 2019): 578–84, https://doi.org/10.2105/AJPH.2018.304904. Thus, state incidences were broken down into three categories: homicides/assaults/shootings by police, suicides/suicide attempts, and unintentional/undetermined intent.
Direct Costs
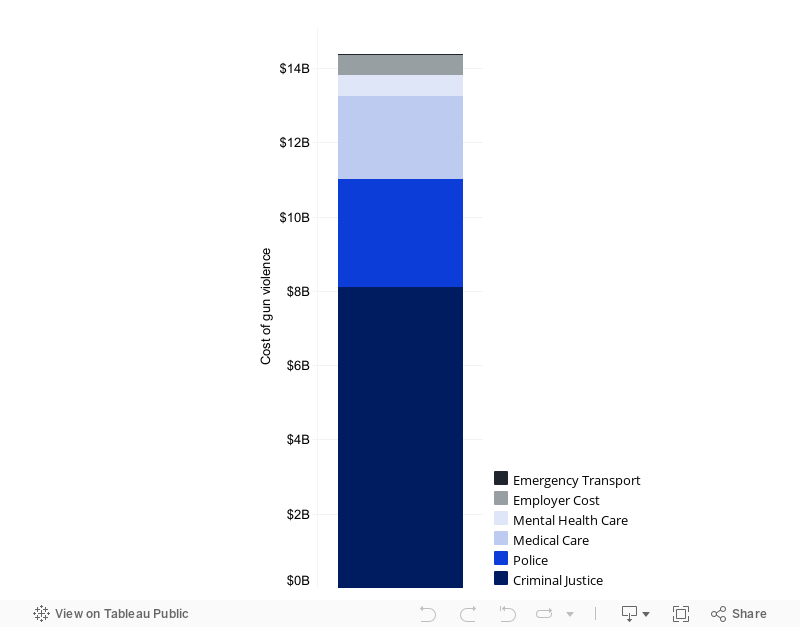
Each year, the direct cost of gun violence is $14.4 billion.
Directly measurable costs are direct expenditures or payments made by individuals, governments, institutions, or corporations for medical bills, government salaries, and other expenditures as itemized in Figure 2.
Figure 2. Direct costs of gun violence
- Criminal justice costs: Direct costs for criminal justice services include costs of court administration, costs of public prosecutors and defenders, and jail and prison incarceration and other sanctions for suspects and perpetrators. Arrest rates from FBI statistics, as well as court and incarceration costs per arrest, use calculations from a 2017 study;9Priscillia Hunt, James Anderson, and Jessica Saunders, “The Price of Justice: New National and State-Level Estimates of the Judicial and Legal Costs of Crime to Taxpayers,” American Journal of Criminal Justice 42, no. 2 (June 1, 2017): 231–54, https://doi.org/10.1007/s12103-016-9362-6. costs of victim assistance were also included.10Kathryn E. McCollister, Michael T. French, and Hai Fang, “The Cost of Crime to Society: New Crime-Specific Estimates for Policy and Program Evaluation,” Drug and Alcohol Dependence 108, no. 1–2 (April 1, 2010): 98, https://doi.org/10.1016/j.drugalcdep.2009.12.002. Criminal justice costs are paid by the government and borne by taxpayers.
- Police costs: Direct costs for police include costs to respond to and investigate firearm incidents that resulted in fatal or nonfatal injuries. Police costs per police-reported crime for murders and nonfatal aggravated assaults are based on a 2019 study.11Priscillia Evelyne Hunt, Jessica Saunders, and Beau Kilmer, “Estimates of Law Enforcement Costs by Crime Type for Benefit-Cost Analyses,” Journal of Benefit Cost Analysis 10, no. 1 (2019): 95–123, https://doi.org/10.1017/bca.2018.19. PIRE assumed that the police costs of investigating a firearm fatality to determine it was not a homicide equaled the costs of investigating a hospital-admitted nonfatal firearm assault. The costs of investigating a hospital-treated nonfatal firearm injury represent eight hours of detective time valued at the national average wage rate for detectives and criminal investigators in 2019,12US Bureau of Labor Statistics, “Occupational Employment and Wages, May 2017,” March 30, 2018, https://www.bls.gov/oes/tables.htm. See “33-3021 Detectives and Criminal Investigators.” Prices were adjusted from 2017 to 2019 using the Consumer Price Index. plus 50 percent to account for fringe benefits and overhead. Costs of police are paid by the government and borne by taxpayers.
- Medical care costs: Direct health-care costs to society include emergency medical care, acute care, rehabilitation, follow-up care, long-term medical and institutional care, prescriptions, ancillary expenses, coroner services, and the costs of health insurance claims processing. PIRE generated average unit costs for treating gunshot wounds in emergency departments and inpatient medical visits, which include specifics about the type and extent of injury and the hospital charge and cost for each visit. Inpatient costs are based on hospital charges and cost-to-charge ratios. Emergency department costs were obtained from estimates made by CDC personnel of mean total costs in the first year for emergency department-treated patients from a 2010–2011 commercial claims database.13The Injury Cost Model develops cost per case using nonfatal injury data coded in the 9th edition of ICD-CM. Therefore, PIRE ran the model on 2014 hospital inpatient and emergency department data to generate the average cost per injury (estimated by severity, intent, and demographics), which was the last full year of data that hospitals coded in ICD-9-CM. See Agency for Healthcare Research and Quality (AHRQ) notes on the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP) and the notes on the Nationwide Emergency Department Sample (NEDS). Selected cases were ICD-9-CM external cause codes of E922.0– E922.4, E922.8, E922.9 (accidental injuries by firearms); E955.0–E955.4, E955.6 (self-inflicted injury by firearms); E965.0–E965.4, E968.6 (assault by firearms); E970.0 (legal intervention involving firearms); E979.4 (terrorism involving firearms); E985.0–E985.4, or E985.6 (injury by firearms, undetermined). As a result, lengths of stay, hospital charges, cost-to-charge ratios, and discharge destinations underlying the Injury Cost Model costs come from 2014 actuals. Each HCUP case was costed based on age, sex,14HCUP and CDC national vital statistics files both report only binary (male or female) sex as indicated on birth or death certificates. anatomic location and nature of the injuries, length of stay for inpatients, and discharge destination. These data were supplemented with Medical Expenditure Panel Survey, IBM MarketScan, and National Council on Compensation Insurance Detailed Claims Information (DCI) data by diagnosis group about physician and other professional fees associated with the hospital visits as well as costs of follow-up care after hospital discharge.
Medical expenses are paid by private payers (families and survivors through private health insurance and out-of-pocket costs); employer costs (e.g., health insurance coverage, employer-paid disability insurance, workers’ compensation); and taxpayers through government programs (e.g., Medicaid, Medicare). - Mental health-care costs: Direct costs for mental health care services include costs to victims or immediate family members seeking treatment from a mental health professional after trauma of firearm injury. Mental health care costs are based on a survey of mental health professionals regarding the proportion of patients receiving treatment in response to violent crime.15Mark A. Cohen and Ted R. Miller, “The Cost of Mental Health Care for Victims of Crime,” Journal of Interpersonal Violence 13, no. 1 (February 1998): 93–110, https://doi.org/10.1177/088626098013001006. It was assumed the mental health burden of a firearm injury did not vary by intent. Mental health care costs are paid by both private payers and by taxpayers through government programs.
- Employer costs: Direct costs to the employer account for productivity losses of victims’ employers, such as the value of the time supervisors spend adjusting schedules to cover for lost work, lost revenues due to unfilled absences, and recruiting and training replacements as necessary. These costs are based on average worker and supervisor wage rates and estimates of time lost by colleagues and supervisors when a worker is temporarily absent or must be replaced.16Ted R. Miller and Maury Galbraith, “Estimating the Costs of Occupational Injury in the United States,” Accident Analysis & Prevention 27, no. 6 (December 1, 1995): 741–47, https://doi.org/10.1016/0001-4575(95)00022-4; Ted R. Miller et al., “Estimating the Cost to Society of Consumer Product Injuries: The Revised Injury Cost Model,” US Consumer Product Safety Commission, January 1998, https://bit.ly/37XqeME. Employer costs are considered to be paid by the private sector.
- Emergency transport costs: Costs for emergency transport include ambulance services and patient transport for initial emergency department treatment and transport if discharged to a health-care facility (e.g., a nursing facility). These costs are included in the Injury Cost Model based on a 2012 Government Accountability Office survey of ambulance providers.17Government Accountability Office, “Ambulance Providers: Costs and Medicare Margins Varied Widely; Transports of Beneficiaries Have Increased,” Report to Congressional Committees, October 2012, https://www.gao.gov/assets/650/649018.pdf. Emergency transport costs are assumed to be paid by taxpayers through government services.
Indirect Costs
Work-Loss Costs
Each year, injuries and deaths from gun violence lead to $53.8 billion in work loss for victims, their families, and, in the case of assaults or homicides, for perpetrators.
Work loss occurs even for unpaid work—for example, household work or caregiving of an injured family member or friend. This forgone work or earnings represent the opportunity costs of time spent away from normal activity as a result of injury or death.
- Survivor work-loss costs: Indirect costs for expected cost of work loss due to firearm injuries and fatalities include wages, fringe benefits, and a wage equivalent for unpaid household work such as caregiving and housekeeping. Work loss includes short-term loss and the present value of a lifetime’s worth of wage and unpaid household/caring work that a person will be unable to do because of death or permanent disability.18Philip J. Cook and Jens Ludwig, Gun Violence: The Real Costs (New York: Oxford University Press, 2000). The projected lifetime earnings losses of firearm decedents are adjusted to be firearm-specific using Cook and Ludwig’s ratios by intent based upon the age and sex distribution of firearm violence victims. Guided by DCI disability data and a published analysis of mortality follow-back data on the income of firearm decedents, the average nonfatal work loss was costed for each nonfatal injury in the HCUP dataset based on age, sex, anatomic location and nature of the injuries, length of stay if admitted as an inpatient, and discharge destination if admitted as an inpatient.19Agency for Healthcare Research and Quality, “Introduction to the HCUP Nationwide Emergency Department Sample (NEDS) 2014,” Healthcare Cost and Utilization Project (HCUP), 2016, https://www.hcup-us.ahrq.gov/db/nation/neds/NEDS2014Introduction.pdf; Agency for Healthcare Research and Quality, “Introduction to the HCUP National Inpatient Sample (NIS) 2014,” Healthcare Cost and Utilization Project (HCUP), 2016, https://www.hcup-us.ahrq.gov/db/nation/nis/NISIntroduction2014.pdf.
- Perpetrator work-loss costs: Costs for projected perpetrators’ work loss were drawn from a 2020 study that calculated this loss similarly to work loss for the person injured or killed (explained above), with adjustments for the age and sex distribution of perpetrators.20Age and sex distribution of the perpetrators were assumed to follow the same patterns as reported by McCollister, French, and Fang, “The Cost of Crime to Society” (April 1, 2010).
Lost Quality of Life
Gun violence injuries and deaths result in $489.1 billion in lost quality of life.
The intention here is not to put a price on life but rather to follow the commonly applied economic models for valuing the intangible loss that victims and survivors of all sorts of injuries and accidents face by placing a dollar value on pain and loss of well-being that a person and their family experience due to either death or injury.
Estimates are based on the Value per Statistical Life lost prescribed by the US Department of Health and Human Services.21US Department of Health and Human Services, Office of the Assistant Secretary for Planning and Education, “Guidelines for Regulatory Impact Analysis,” 2016, https://aspe.hhs.gov/sites/default/files/migrated_legacy_files//171981/HHS_RIAGuidance.pdf; Gabrielle F. Miller et al., “Monetised Estimated Quality-Adjusted Life Year (QALY) Losses for Non-fatal Injuries,” Injury Prevention (online print ahead of publication, March 16, 2022), https://doi.org/10.1136/injuryprev-2021-044416. Quality-of-life costs exclude work losses to avoid double counting. “Quality of life lost” represents the present value of what was lost because of a life cut short or a person was permanently disabled by gun violence. As a result, fatal injuries account for most of the quality of life lost. Deaths of young persons result in greater loss. Similar to the medical health-care costs, the average nonfatal quality-of-life costs were estimated for each HCUP case based on age, sex, anatomic location and nature of the injuries, and length of stay and discharge destination if admitted as an inpatient. Thus, the quality-of-life costs were adjusted for age-, sex-, and survival-specific data and averages constructed based on population weighting.
Government Costs Paid by Taxpayers
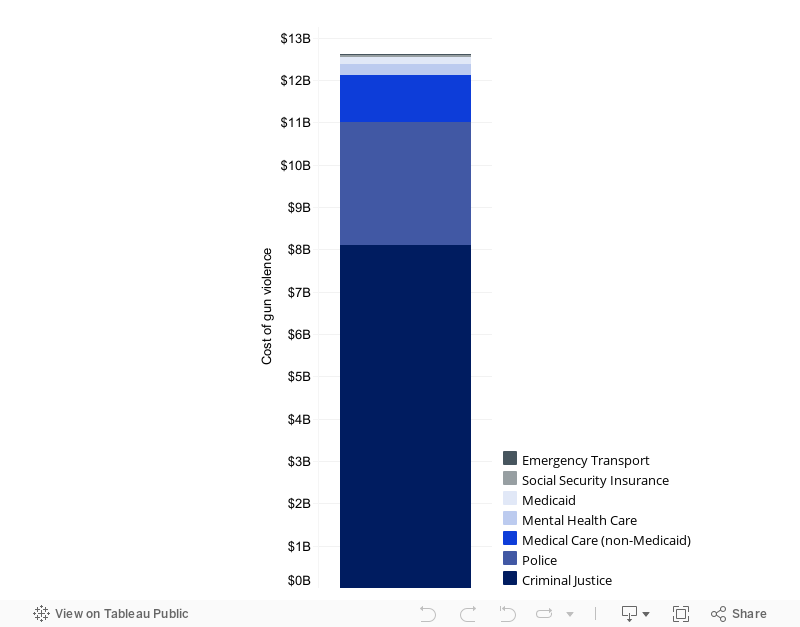
Each year, injuries and deaths from gun violence cost the federal, state, and local governments a total of $12.6 billion.
The government cost of gun violence paid by taxpayers was calculated as the sum of the government share of expenditures in six major categories: medical and mental health-care treatment for firearm injuries and deaths; emergency transport; police response; criminal justice; Medicaid for general (non-firearm-related) health care; and federal Supplemental Security Income (SSI) payments, also referred to as Social Security insurance.
Figure 3. Government costs, paid by taxpayers
- Criminal justice, police, and emergency transport: The full amounts of direct costs for these three categories were included as government costs, borne by taxpayers; it was assumed that private payers do not contribute to these costs.
- Medical and mental health care: The share of direct medical costs paid by government (i.e., Medicare and Medicaid) was extracted from the 2014 HCUP datasets22Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project (HCUP), “HCUP National Inpatient Sample (NIS),” https://www.hcup-us.ahrq.gov/db/nation/nis/nisdbdocumentation.jsp; “HCUP Nationwide Emergency Department Sample (NEDS).” Data from 2014. from actual charges and payments for firearm injuries (by intent, severity, and demographics of the injured) at the hospitals surveyed; the same percentage share was applied for mental health-care costs.
- Medicaid for general health care: Direct costs for Medicaid payments for non-firearm-related health care were included in government costs of firearm violence based on the fact that if a person became eligible for Medicaid based on firearm injury, that person also is covered by Medicaid for general health-care costs.23Eduard Zaloshnja et al., “How Often Do Catastrophic Injury Victims Become Medicaid Recipients?,” Medical Care 50, no. 6 (2012): 513–19; Michael Smith, Ted R. Miller, and Eduard Zaloshnja, “Enduring Enrolments in West Virginia’s Medicaid Programme Due to Severe Injury,” Injury Prevention 24, no. 5 (October 1, 2018): 332–36, https://doi.org/10.1136/injuryprev-2017-042373. Medicaid for general health care is not included in the direct costs for medical expenses because it is not the cost of treatment of a firearm injury.
- Supplemental Security Income (SSI): The direct cost of a fixed monthly payment for SSI was added to the government cost for a subset of persons injured by firearms who are estimated to remain on Medicaid permanently until age 65.24Smith, Miller, and Zaloshnja, “Enduring Enrolments in West Virginia.” SSI is a government payment (and therefore a direct expenditure) to eligible individuals; its purpose is to help offset the indirect and intangible costs such as loss of work and quality of life. SSI costs were not included in the direct costs because they are government transfers to offset the work-loss and intangible costs.
PIRE’s estimate of the government costs for fatal and nonfatal firearm injuries, in order to be conservative, excluded tax revenue loss. Forgone taxes on earnings lost by firearm injury victims were not included in the total costs of gun violence to the government. Rather, it was conservatively assumed that when someone loses work or leaves the workforce because of firearm injury, someone else replaces that worker, and therefore the potential lost tax revenue from lost wages is minimal.25Edward M. Gramlich, Benefit-Cost Analysis of Government Programs (Englewood Cliffs, NJ: Prentice Hall, 1981); Marc A. Koopmanschap et al., “The Friction Cost Method for Measuring Indirect Costs of Disease,” Journal of Health Economics 14, no. 2 (June 1995): 171–89, https://doi.org/10.1016/0167-6296(94)00044-5.
Additionally, the PIRE model is limited to the cost of injuries and therefore excludes potential property tax revenue loss from property values declining or sales tax loss from business in a community declining in response to gun violence in the community.26Yasemin Irvin-Erickson et al., “Gun Violence Affects the Economic Health of Communities,” Urban Institute, June 2, 2017, https://www.urban.org/research/publication/gun-violence-affects-economic-health-communities; Nicole Weissman, “Is Gun Violence Stunting Business Growth?,” Urban Institute, November 3, 2016, https://www.urban.org/features/gun-violence-stunting-business-growth.
Everytown Research & Policy is a program of Everytown for Gun Safety Support Fund, an independent, non-partisan organization dedicated to understanding and reducing gun violence. Everytown Research & Policy works to do so by conducting methodologically rigorous research, supporting evidence-based policies, and communicating this knowledge to the American public.
